What You Need to Know About Medicare Site-Neutral Payment Reform
Today, the vast majority of Traditional Medicare’s payments for outpatient care differentiate between outpatient settings, usually paying more for the same service when it is provided in a hospital outpatient department (HOPD). In response to concerns that this is driving up unnecessary spending and encouraging consolidation, Congress and federal officials have taken steps to apply site-neutral payment principles to outpatient services in limited circumstances. Several proposals currently seek to expand Medicare’s use of site-neutral payment. This guide offers a snapshot of these efforts.
Curious about commercial health insurance?
Medicare’s efforts inform a growing interest in adopting site-neutral reforms to the commercial market. Explore our resource Site-Neutral Payment Reform and the Commercial Market for more information.
Customary Outpatient Payment Rules in Medicare
Traditional Medicare (i.e., Medicare Parts A and B) pays most hospitals for outpatient services under the outpatient prospective payment system (OPPS) and pays health care professionals under the Physician Fee Schedule, regardless of where the service was provided. When a Medicare beneficiary receives care in an HOPD, Medicare typically pays the health care professional providing care under the PFS and pays the facility under the OPPS. Similarly, when Medicare enrollees go to an ambulatory surgery center (ASC) for outpatient care, Medicare pays the professional’s fee under the Physician Fee Schedule and pays the ASC under the ASC payment system. In these instances, Medicare reduces the practice expense portion of the Physician Fee Schedule, since it is now paying the facility for these overhead costs. Nevertheless, Medicare’s total payment for care at an HOPD or an ASC is higher than its Physician Fee Schedule payment for care in a freestanding physician office, which does not receive a separate facility payment.
Current Site-Neutral Payment Rules in Medicare
Through a mix of congressional and agency action, Medicare has begun reducing OPPS payments for a very limited set of services so that the total payment for a service delivered at an HOPD is equivalent to the Physician Fee Schedule payment for the same care in a freestanding office.
Under the Bipartisan Budget Act of 2015 (BBA 2015), off-campus HOPDs that began providing services on or after November 2, 2015—“non-excepted” off-campus HOPDs—are paid on a site-neutral basis for all services. Under payment rules issued by the Centers for Medicare & Medicaid Services (CMS), the remaining “excepted” off-campus HOPDs are paid on a site-neutral basis for clinic visits only.
Site-neutrality reforms still do not generally apply to on-campus services. In addition, several types of hospitals and settings, including dedicated emergency departments, certain cancer hospitals, critical access hospitals, rural sole community hospitals, and rural emergency hospitals, are unaffected by Medicare site-neutral rules.
Altogether, only 1.5 percent of Medicare spending on services delivered in HOPDs was paid on a site-neutral basis as of 2022. (See Figure 1.)
Figure 1
$807 Million (1.5%) of Annual Medicare HOPD Spending Was Site Neutral in 2022
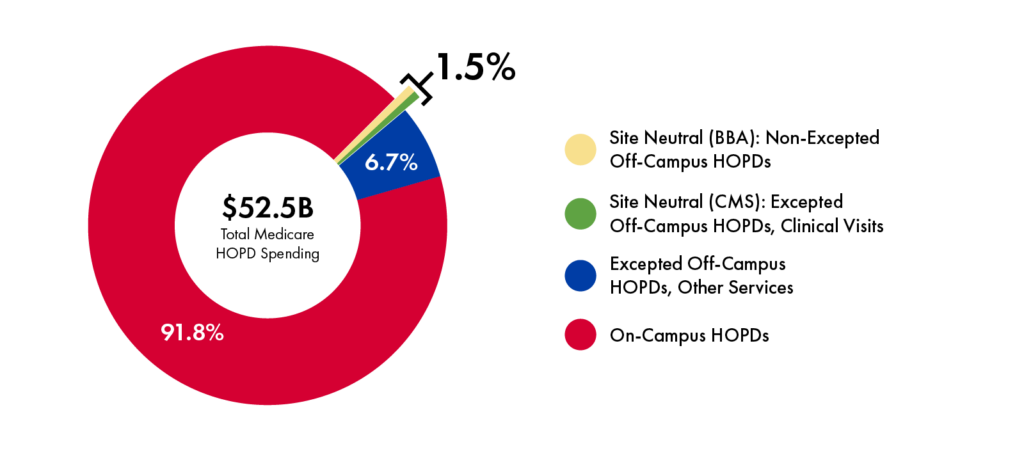
CMS extended its site-neutral payments to outpatient physician administration of drugs in excepted off-campus HOPDs beginning in 2026. CMS estimates this change will realize $290 million in savings in its first year, with the savings split between Medicare spending ($220 million) and beneficiary cost-sharing ($70 million).

Inherently Site-Neutral Services
Medicare pays some services using the Physician Fee Schedule rate regardless of whether patients receive them in an HOPD, ASC, or freestanding setting. This means there is no site-of-service difference in payment rates. These services include mammography, physical therapy, occupational therapy, and wellness visits.
MedPAC Recommendations
The Medicare Payment Advisory Committee (MedPAC) has recommended that Medicare payment rates across outpatient settings align more closely for “selected services that are safe and appropriate to provide in all settings and when doing so does not pose a risk to access.” This recommendation would apply to both on- and off-campus HOPDs.
To identify appropriate services for this policy, MedPAC sorted services into ambulatory payment classifications (APCs), which are sets of clinically similar groups of services that are paid the same amount under the OPPS. For each APC, MedPAC calculated the frequency with which each APC was provided in an HOPD, ASC, or freestanding physician office between 2016 and 2021 (excluding 2020).
Exclusions from MedPAC’s Site-Neutral Payment Recommendation
MedPAC excluded two types of APCs from its analysis for which it determined differential payments are appropriate:
- MedPAC excluded APCs for emergency department and trauma care, which depend on standby emergency capacity and impose additional costs on providers.
- MedPAC excluded six APCs where the primary service included within the APC was commonly bundled with other ancillary items or services, and these ancillary items or services were frequently provided in HOPDs rather than freestanding physician offices.
After excluding certain APCs from its analysis (see box above), MedPAC found that 57 APCs were most commonly performed at freestanding physician offices, and identified 9 APCs for which volume was highest at ASCs. (See Figure 2.)
MedPAC reasoned that APCs that were most frequently provided in freestanding physician offices could be safely provided in a freestanding physician office to most beneficiaries. Accordingly, it would be reasonable to align OPPS and ASC payment rates with the Physician Fee Schedule for those APCs. Likewise, APCs that were most frequently provided in an ASC could be safely provided in an ASC to most beneficiaries and it would be reasonable to align OPPS payment rates with the ASC payment rate for those services. (Freestanding physician offices would still be paid the Physician Fee Schedule rate in such circumstances.)
MedPAC used this list of services to estimate the savings potential for site-neutral payment in Medicare, basing payment amounts on the amount paid to the most common setting for each APC. However, MedPAC observed that clinical perspectives and the potential for unintended consequences should also inform decisions about which services are appropriate for site-neutral payment.
Figure 2.
MedPAC-Identified Illustrative Services for Aligning Fee-For-Service Payments Between Outpatient Hospitals and Physician Offices and ASCs
| APC Description | Program Spending, 2021 (in millions) | Beneficiary Cost Sharing, 2021 (in millions) |
|---|---|---|
| Physician Office Imaging | ||
| Imaging w/o Contrast: Levels 1–4 | $2,312 | $578 |
| Nuclear Medicine: Level 3 | 642 | 160 |
| Physician Office Evaluation and Management (E&M) | ||
| Clinic Visits | 2,056 | 514 |
| Health and Behavior Services: Levels 1–3 | 154 | 38 |
| Physician Office Treatments | ||
| Drug Administration: Levels 1–4 | 2,031 | 508 |
| Nerve Injections: Levels 1–3 | 627 | 159 |
| Therapeutic Radiation Treatment Preparation: Level 1 | 136 | 46 |
| Radiation Therapy: Level 1 | 1 | 0.3 |
| Manipulation Therapy | 0.5 | 0.1 |
| Physician Office Procedures | ||
| Skin Procedures: Levels 1–5 | 726 | 183 |
| Urology and Related Services: Levels 1–3 | 343 | 85 |
| Minor Procedures: Levels 1–5 | 180 | 45.3 |
| Excision/Biopsy/Incision and Drainage: Level 1 | 76 | 19 |
| Strapping and Cast Application: Level 1 | 51 | 13 |
| Airway Endoscopy: Level 1–3 | 68 | 16 |
| Ear, Nose, and Throat Procedures: Levels 1–4 | 47 | 12 |
| Laser Eye Procedures | 20 | 5 |
| Musculoskeletal Procedures: Level 1 | 10 | 2 |
| Gynecologic Procedures: Levels 1–3 | 12 | 3 |
| Extraocular, Repair, and Plastic Eye Procedures: Levels 1–2 | 4 | 2 |
| Physician Office Tests | ||
| Diagnostic Tests and Related Services: Levels 1–4 | 446 | 111 |
| Pathology: Level 1 | 31 | 8 |
| Physician Office —Other | ||
| Electronic Analysis of Devices: Levels 1–3 | 38 | 10 |
| ASC Procedures | ||
| Lower Gastrointestinal Procedures: Levels 1–2 | 940 | 235 |
| Intraocular Procedures: Levels 1–2 | 780 | 195 |
| Nerve Procedures: Level 1 | 221 | 55 |
| Musculoskeletal Procedures: Level 2 | 92 | 23 |
| Neurostimulator and Related Procedures: Level 2 | 69 | 17 |
| Extraocular, Repair, and Plastic Eye Procedures: Levels 3–4 | 53 | 13 |
| Note: “Program spending” indicates outlays by the Medicare program and excludes beneficiary cost sharing. For all APCs except one, “beneficiary cost sharing” is 25 percent of program spending. Source: June 2023 Report to the Congress: Chapter 8: Aligning Fee-For-Service Payment Rates Across Ambulatory Settings,” MedPAC (June 2023), https://www.medpac.gov/wp-content/uploads/2023/06/Jun23_Ch8_MedPAC_Report_To_Congress_SEC.pdf. | ||
Medicare Site-Neutral Payment Reform Proposals
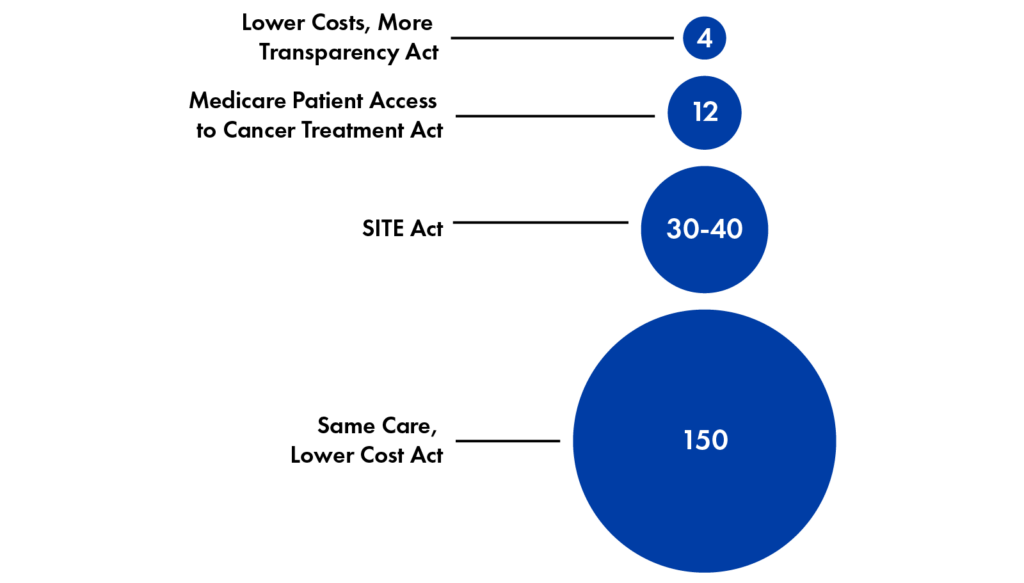
Members of Congress have proposed an array of Medicare site-neutral payment reform bills, which vary in scope and potential savings. (See Figure 3.) These proposals include:
- Outpatient physician administration of drugs at on- and off-campus HOPDs (Lower Costs, More Transparency Act)
- Outpatient cancer care at off-campus HOPDs (Medicare Patient Access to Cancer Treatment Act)
- All services at off-campus HOPDs (SITE Act)
- All MedPAC-identified services and any other codes the Secretary of Health and Human Services deems appropriate, at on- and off-campus settings (Same Care, Lower Cost Act)
Figure 3
Estimated Federal Savings for Site-Neutral Bills over 10 Years ($ in Billions), from
Various Sources
Sources: Congressional Budget Office, “Estimated Direct Spending and Revenue Effects of H.R. 5378, the Lower Costs, More Transparency Act,” 2023; American Hospital Association, “Fact Sheet: Medicare Site-Neutral Legislative Proposals Under Consideration Would Jeopardize Access to Care for Patients and Communities,” 2023; Committee for a Responsible Federal Budget (CFRB), “Key Takeaways from the Site-Based Invoicing and Transparency Enhancement (SITE) Act,” 2023; Actuarial Research Corporation, “Updated Estimates of Site Neutrality and Evaluation of the Cassidy-Hassan Framework,” 2025; CFRB, “New Site-Neutral Bill Introduced in Senate,” 2025
Senators Cassidy and Hassan’s 2024 white paper outlines policy options to advance Medicare site-neutral payments while reinvesting savings in rural and safety net hospitals. Their approach would establish site-neutral payments for all services at off-campus HOPDs and, at on-campus HOPDs, any services identified using a MedPAC-style analysis. The senators have not yet released legislative language to execute their ideas.
Implications for Commercial Insurance
Innovations in Medicare payment policy have seeded changes in commercial health insurance reimbursement, such as the use of diagnosis-related groups for inpatient care. Similarly, should Medicare adopt further site-neutral payment reforms, supporters argue that these changes may help reduce differences in commercial outpatient payments because commercial payers frequently use Medicare to guide their reimbursement rates. Research suggests that Medicare site-neutral reforms are unlikely to eliminate commercial site-based payment differences, however, since commercial market rates tend to follow the direction, but not the magnitude, of Medicare payment rate changes. Since private insurance is the largest purchaser of ambulatory services, payment reforms that target commercial payers, and address the particular dynamics of the commercial market, will be critical to controlling spending on outpatient care.
Read our policy framework for site-neutral payment reform in the commercial market to explore the options.About
Authors: Christine H. Monahan, Karen Davenport, Julia Burleson, and Kennah Watts
Published April 2026
This work was completed in partnership with West Health.